Patient Support Strategies
Supporting the Patient: A Critical Element of Care
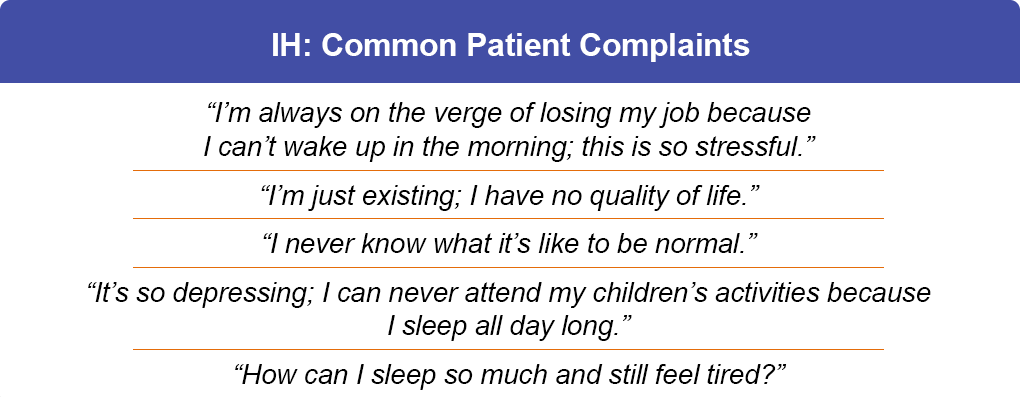
Major Burdens of IH
Major deficits in cognitive, emotional, relational, and functioned outcomes were characterized in the Real-World Idiopathic Hypersomnia Outcomes Study (ARISE), which identified major reductions in these and other parameters.1 Indeed, approximately 2/3 of the patients reported cognitive complaints and moderate to severe depression symptoms. IH has been associated with a high comorbidity burden, including sleep apnea, pain, mood disorders, and several cardiovascular conditions such as hypertension, hyperlipidemia, cardiovascular disease, and stroke.2 IH was also associated with absenteeism, presenteeism, reduced overall work productivity, and reduced ability to perform regular daily activities—all of which reduced overall quality of life substantially.1 As a result, several avenues of patient support are needed to most effectively manage IH.3

Symptom Support
While all patients with IH experience EDS, the presence and severity of other symptoms vary. A study showed that daily EDS was self-reported by 98% of participants, brain fog by 83%, sleep inertia by 79%, and long sleep time (LST; sleeping >10 hours at a time or requiring a nap) by 51%.4 Autonomic symptoms may also be present in idiopathic hypersomnia; these include headache, orthostatic hypotension, temperature imbalance, and peripheral vascular symptoms (eg, Raynaud syndrome).2 As a result each patient needs to be supported based on their individual symptoms and considerations.

Comorbidity Support
Many patients with IH present with comorbidities. Research shows that patients with IH are more likely to have sleep apnea, hypertension, hyperlipidemia, diabetes, mood disorders, and headache/migraine than individuals in reference populations.5
Lifestyle Support
Current guidelines for managing IH recommend assessing and incorporating patient preferences and values when establishing the best treatment plan. Those close to the patient—family, friends, teachers, coworkers—may mistake sleepiness for inattention or other emotions. Patient lifestyle and treatment cost should also inform initial treatment decisions and decisions after treatment failure.3

Satisfaction Support
Patients with IH often voice treatment dissatisfaction, primarily driven by dissatisfaction with treatment effectiveness.6 In 1 study the most common off-label classes of prescription medications used for IH were stimulants (61.3%), wake-promoting agents (28.0%), and antidepressants (18.7%), while nonprescription measures included caffeine (73.3%), planned naps (34.7%), and individual accommodations (32.0%).6 Delivering effective treatment based on individual patient factors should be a critical aspect of IH management.

References
- Stevens J, Schneider LD, Husain AM, et al. Impairment in functioning and quality of life in patients with idiopathic hypersomnia: the Real-World Idiopathic Hypersomnia Outcomes Study (ARISE). Nat Sci Sleep. 2023;15:593-606.
- Saad R, Markt SC, Lillaney P, et al. The clinical and economic burden of idiopathic hypersomnia and narcolepsy: A United States claims-based analysis. Nat Sci Sleep. 2025;17:1809-1823.
- Thorpy M, Krahn L, Ruoff C, et al. Clinical considerations in the treatment of idiopathic hypersomnia. Sleep Med. 2024;119:488-498.
- Trotti LM, Ong JC, Plante DT, et al. Disease symptomatology and response to treatment in people with idiopathic hypersomnia: initial data from the Hypersomnia Foundation registry. Sleep Med. 2020;75:343-349.
- Saad R, et al. Characteristics of adults newly diagnosed with idiopathic hypersomnia in the United States. Sleep Epidemiol. 2023;3:100059.
- Schneider LD, Stevens J, Husain AM, et al. Symptom severity and treatment satisfaction in patients with idiopathic hypersomnia: the Real-World Idiopathic Hypersomnia Outcomes Study (ARISE). Nat Sci Sleep. 2023;15:89-101.
All URLs accessed September 2, 2025