Assessment
Tools for Assessment and Diagnosis of IH
Best Practices for IH Diagnosis
Making a diagnosis of IH involves a careful clinical history, with particular attention to the possibility of other disorders with similar symptomatology, and objective testing with actigraphy, polysomnography, and multiple sleep latency testing.
According to the International Classification of Sleep Disorders (ICSD), third edition, the diagnostic criteria for IH are as follows:1,2
- Patient has daily periods of irrepressible need to sleep or daytime lapses into drowsiness or sleep occurring for at least 3 months
- Cataplexy is absent
- Fewer than 2 sleep-onset rapid eye movement periods (SOREMPs) or no SOREMPs if the REM latency on the preceding nocturnal polysomnography was ≤15 minutes
- PSG and MSLT findings are not consistent with a diagnosis of narcolepsy type 1 or 2
- Presence of at least 1 of the following:
- MSLT, performed in accordance with current recommended protocols, shows a mean sleep latency of ≤8 minutes
- Total 24-hour sleep time ≥660 min (typically 12–14 hours) on 24-hour PSG (performed after correction of chronic sleep deprivation) or wrist actigraphy in association with a sleep log (averaged over at least 7 days with unrestricted sleep)
- Insufficient sleep is ruled out (if deemed necessary, by lack of improvement of sleepiness after an adequate trial of increased nocturnal time in bed, preferably confirmed by at least a week of wrist actigraphy)
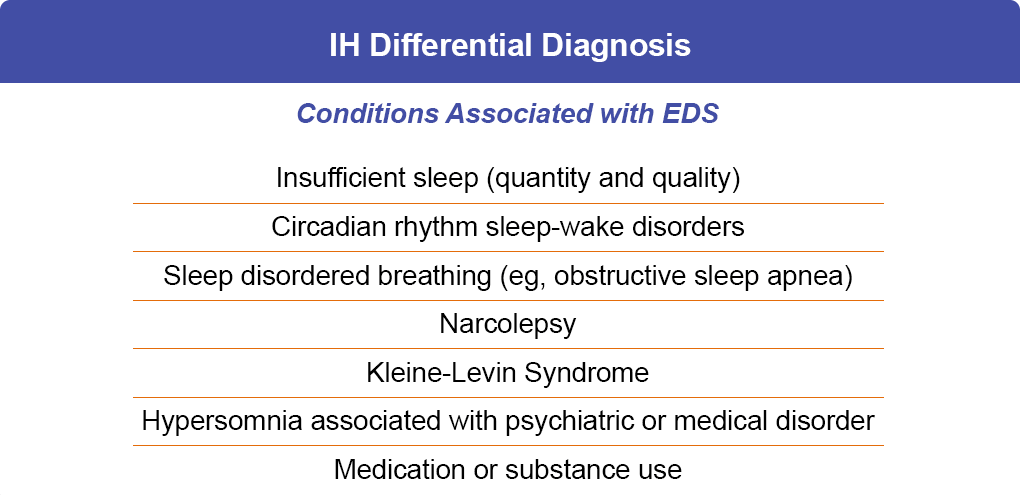
When comparing IH and narcolepsy type 1 (NT1; Table 1 below), the differences are fairly straightforward with regard to cataplexy, sleep quality, and naps. However, the distinction between IH and narcolepsy type 2 (NT2) can be considerably more difficult. Cataplexy is absent in both disorders, and other components of the “narcolepsy tetrad” (ie, sleep paralysis and sleep-related hallucinations) are commonly seen in patients with NT2 and about 1/4 of patients with IH. As a result, these features are not useful for ruling out a diagnosis of IH. Additionally, similar to IH, long sleep times may be present in NT2.3 As a result of this symptom overlap, the differentiation between IH and NT2 rests entirely on the presence or absence of at least 2 sleep-onset rapid eye movement periods (SOREMs) on PSG/MSLT (with 0–1 SOREMs in patients with IH).

Once established, IH is usually stable and long-lasting; however, fluctuations in disease severity may be observed as documented by changes in MSLT results over multiple year intervals and spontaneous remissions reported in several series.4,5 The spectrum of IH and fluctuations in disease require that the individual with IH be continually monitored and followed over the long term to ensure appropriate management.6
Diagnostic Challenges
Patients often describe their sleepiness using vague terms such as “tired,” “fatigue,” or “lack of energy.”7 For clinicians it is important to distinguish between sleepiness and fatigue. Fatigue is a physical or psychological feeling that may occur in a variety of other disorders, such as depression or Parkinson disease. Unlike sleepiness, patients who are fatigued do not fall asleep when involved in sedentary activities such as watching television or reading. This distinction is important because “sleepiness” indicates the presence of a sleep disorder or a problem with nighttime sleep. Patients may or may not be aware of their sleepiness before falling asleep, but it often significantly affects their quality of life. The Epworth Sleepiness Scale (ESS) can assist with the screening of individuals as the scores significantly distinguished normal subjects from patients in various diagnostic groups including obstructive sleep apnea syndrome, narcolepsy, and IH.8
The results of the Real World Idiopathic Hypersomnia Outcomes Study (ARISE) showed that IH has a large impact on different areas of life, such as daily functioning, activities, thinking, mood, relationships and work.9 As a result, clinicians may experience difficulty in diagnosis based on the constellation of signs and symptoms as well as impact on daily life. As onset of narcolepsy and IH may be gradual, a diagnosis may not occur until a catastrophic event due to sleepiness, such as a car accident or reduced work productivity, which leads to patient presentation in the clinic.
References
- Dhillon K, Sankari A. Idiopathic hypersomnia [updated 7/31/2023]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025.
- American Academy of Sleep Medicine (AASM). International Classification of Sleep Disorders. 3rd ed, text revision. 2023.
- Vernet C, Arnulf I. Narcolepsy with long sleep time: a specific entity? Sleep. 2009;32:1229-1235.
- Bassetti C, Aldrich M. Idiopathic hypersomnia. A series of 42 patients. Brain. 1997;120:1423-1435.
- Billiard M, Merle C, Carlander B, et al. Idiopathic hypersomnia. Psychiatr Clin Neurosci. 1998;52:125-129.
- Trotti L. Idiopathic hypersomnia. Sleep Med Clin. 2017;12:331-344.
- Monderer R, Ahmed IM, Thorpy M. Evaluation of the sleepy patient: differential diagnosis. Sleep Med Clin. 2017;12:301-312.
- Johns M. A new method for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep. 1991;14: 540-545.
- Stevens J, Schneider LD, Husain AM, et al. Impairment in functioning and quality of life in patients with idiopathic hypersomnia: The Real World Idiopathic Hypersomnia Outcomes Study (ARISE). Nat Sci Sleep. 2023;15:593-606.